

")

Headaches
In most cases, headaches require an exhaustive case history, experience, specific diagnostic procedures, and often also patience, but they can be effectively treated. Headaches can have a large variety of causes and characteristics. Keeping a pain diary in cases of chronic pain will be useful. The most important types of headaches we treat include:
Migraine
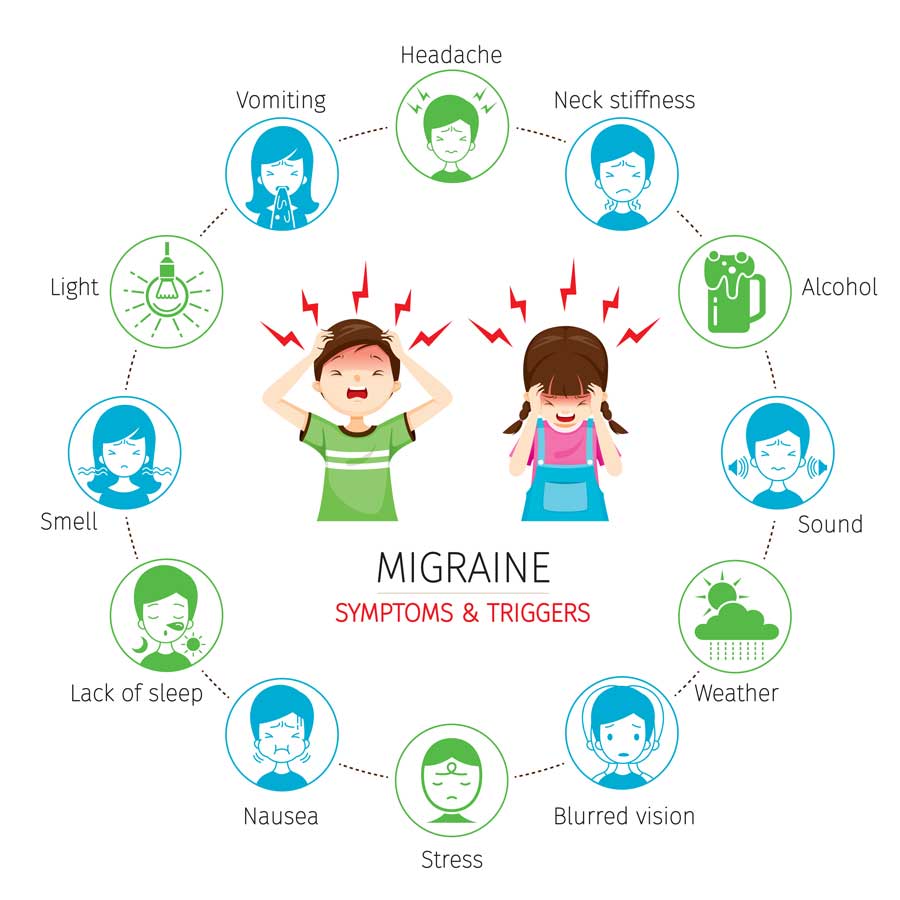
A migraine is a severe, pulsating headache that usually occurs relatively suddenly and is often felt on one side of the head. Migraine is often accompanied by symptoms such as photophobia and sensitivity to noise, nausea, and vomiting. The individual migraine attack can be accompanied by a so-called aura. This can cause visual, sensory, motor and occasionally also speech dysfunction.
In cases of frequent migraine attacks, pharmacological prevention with drugs, including botulinum toxin is possible. Now, a treatment with monoclonal antibodies is even possible, by means of which a lasting significant improvement can be achieved in a large number of patients.
Tension headaches
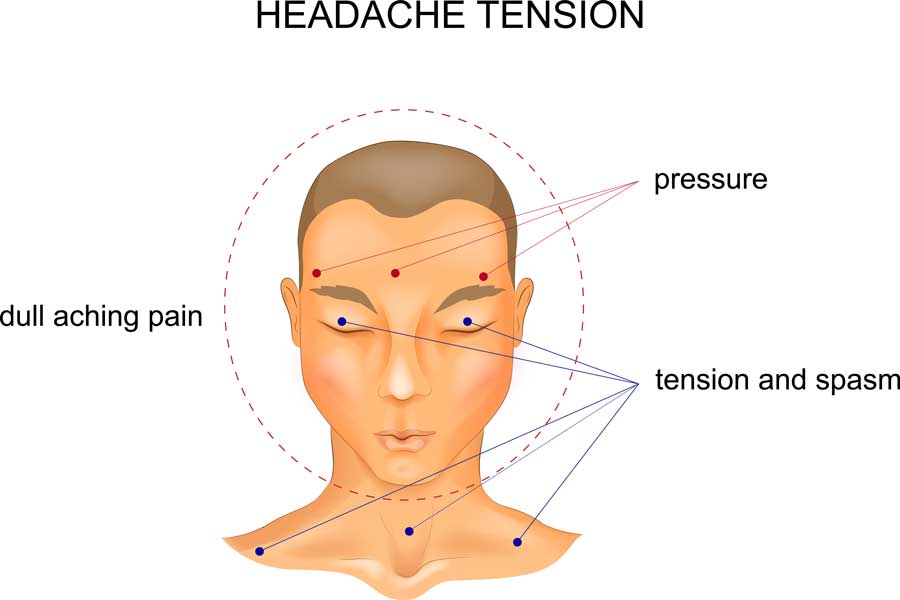 This form of headache can be episodic or chronic. The pain occurs in the entire head and is of a pressing or tearing nature. Mild to moderate pain that mostly does not increase with exertion can last from some minutes to several days. In addition to common pain-relieving medication in the form of tablets, this pain can often be treated by means of a specific infiltration of the cervical spine and head. Thus, we also apply pain therapy with botulinum toxin. Particularly in the case of tension headaches, injections of this medication into the neck and chewing muscles can lead to relaxation, which then results in a relief of the pain.
This form of headache can be episodic or chronic. The pain occurs in the entire head and is of a pressing or tearing nature. Mild to moderate pain that mostly does not increase with exertion can last from some minutes to several days. In addition to common pain-relieving medication in the form of tablets, this pain can often be treated by means of a specific infiltration of the cervical spine and head. Thus, we also apply pain therapy with botulinum toxin. Particularly in the case of tension headaches, injections of this medication into the neck and chewing muscles can lead to relaxation, which then results in a relief of the pain.
Cluster headache
 Cluster headache is the term used to describe most intense, severe hemifacial attacks of pain that always affects the same side of the head. Several such attacks can occur on a daily basis, lasting from a few minutes to a few hours. The pain is perceived as burning or stabbing, occasionally also as a burning pain. It is frequently accompanied by psychomotor restlessness and reddened eyes, nasal congestion and watery eyes.
Cluster headache is the term used to describe most intense, severe hemifacial attacks of pain that always affects the same side of the head. Several such attacks can occur on a daily basis, lasting from a few minutes to a few hours. The pain is perceived as burning or stabbing, occasionally also as a burning pain. It is frequently accompanied by psychomotor restlessness and reddened eyes, nasal congestion and watery eyes.
Dizziness and vertigo

The sensation of spinning or swaying, the feeling of not being able to move safely in a room, or even the feeling of impending unconsciousness is not only an unpleasant but often frightening experience for most people. In medical terms, vertigo is defined as a perceived apparent movement between oneself and the environment. A distinction is made between, among others, spinning, swaying, lifting, motion and unsystematic vertigo. Dizziness is experienced in the head.
It is not a disease in the actual sense, but a multifaceted syndrome, a syndrome that can be very stressful to those affected and in part may even be dangerous due to the risk of falling. Dizziness can occur in attacks or permanently. It can appear as a spinning or swaying sensation, unsteady gait, or as light-headedness. Dizziness can be a symptom of a harmless and easily treatable disease, but it can also be the first symptom of a dangerous circulatory disorder in the brain. Since dizziness is often experienced with a high degree of anxiety, psychological factors may also contribute.
Effective therapies are available for most forms of vertigo. The aim is to identify the patient's specific vertigo based on an individual description of the symptoms and a precise physical examination. You can find a diary here to document a possibly existing vertigo. In terms of diagnosis and therapy, the patients can benefit from modern interdisciplinary diagnostic procedures (ophthalmology, neuroradiology, internal medicine, orthopedics).
Head movements, lying down or turning over in bed, getting up from lying or sitting, bending, walking - all these movements can trigger vertigo. Vertigo is frequently accompanied by symptoms like nausea or vomiting, headache, hearing disorders, double vision, sensitivity to light or noise. The type and duration of the vertigo attacks often give the physician important clues about the cause of the vertigo.
- The most common is benign, suddenly occurring (=paroxysmal) positional vertigo, which is in principle a harmless, but often not properly recognized, form of vertigo. The origin of vertigo lies in the organ of balance. In this case, small calcium stones in the inner ear get into the wrong place in the organ of equilibrium, the semicircular canals system, and deliver false signals to the brain in strict dependence on rapid head movements. Vertigo is usually triggered by jerky head movements, for example in the morning when waking up or getting out of bed. If the clinical picture is understood correctly, the therapy of benign positional vertigo is uncomplicated. With a special sequence of movements and positioning of the body, the "ear stones" can be brought back to their original position. In most cases, the vertigo then quickly disappears. It is one of the simplest, cheapest, and most effective procedures in medicine at all which is unfortunately still used too rarely.
- Cerebral blood supply disorders are often manifested by dizziness; in this case, appropriate diagnostic procedures are important to prevent the onset of strokes.
Chronic pain

Patients with chronic pain may develop a so-called pain behavior due to the lasting pain. You can find a pain diary for documentation here...
Typical signs:
- pronounced protective posture
- hyper- or hypoactivity
- depressive mood
- fears
- little endurance and little motivation
- impaired self-confidence and diminished self-esteem
- social withdrawal
- disturbed action abilities
- sleep, dizziness, and appetite disorders
- metabolic symptoms (e.g. heavy sweating)
- income or job problems, up to and including their loss.
The aim is to change the perception as well as the behavior, such that the patient's quality of life is improved. This can, and also should, be multidisciplinary. In this respect, we can count on a good interdisciplinary collaboration with the departments of orthopedics and traumatology (Dr. Patrick Garcia), psychology, and physiotherapy (Palma-Vital) in our practice.
Stroke
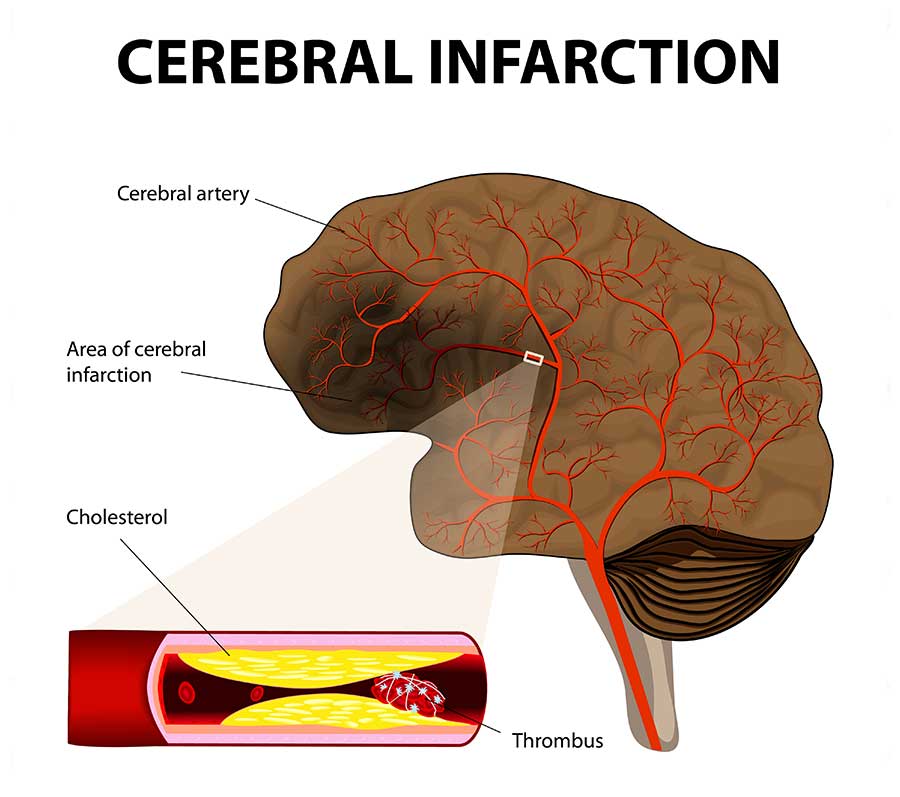 The faster an acute stroke is treated, the less permanent is the damage. That's where the maxim "Time is Brain" comes from. The brain tissue, which no longer receives sufficient oxygen due to a vascular occlusion, should be resupplied with blood by thrombolysis or thrombectomy before it dies.
The faster an acute stroke is treated, the less permanent is the damage. That's where the maxim "Time is Brain" comes from. The brain tissue, which no longer receives sufficient oxygen due to a vascular occlusion, should be resupplied with blood by thrombolysis or thrombectomy before it dies.
As signs of a stroke, several symptoms can occur suddenly, and, depending on the severity, also simultaneously:
- numbness in the face, an arm, leg or an entire side of the body,
- confusion, speech or word finding, writing or comprehension disorder,
- swallowing disorders (dysphagia),
- painless visual disorder in one or both eyes, one-sided pupil dilation, visual field failure, double vision,
- vertigo, gait disturbance, balance or coordination disorder (ataxia),
- lack of perception of part of the environment or of one's own body,
- disturbed consciousness (somnolence, coma), orientation disorders,
- severe headache, nausea and vomiting,
- may indicate a cerebral hemorrhage.
An acute stroke is an emergency case and must be immediately treated in the hospital (s. below in-hospital acute treatment). After a stroke, further neurological care is usually necessary, for example, for pharmacological therapy, for palsies, or for epileptic seizures.
Transient ischemic attacks (TIA) are short blood supply disorders that result in temporary neurological deficits. As they are harbingers of stroke, further examinations must be carried out in order to minimize the risk of a subsequent stroke. In the case of narrowed brain-supplying arteries (e.g. carotid stenosis), regular checks by means of state-of-the-art ultrasound procedures are carried out in our practice in order to prevent a stroke, but also to prevent unnecessary procedures on the blood vessels (s. below color-coded Doppler and duplex sonography of the neck vessels and brain arteries).
Parkinson's disease
The movements of the body are controlled and coordinated by specialized neuron clusters in the brain. An outstanding role for the control and fine-tuning of movement sequences is played by an extensive core area in the center of the cerebrum, the "basal ganglia".
The most frequent symptoms occurring as a consequence of a functional disturbance of the basal ganglia is Parkinson's disease.
Parkinson's disease manifests itself as, frequently asymmetrical, akinesia (poverty of movement) with bradykinesia (slowness of movement), postural instability and resting and postural tremor. Often, there are also multiple non-motor symptoms such as autonomic dysfunctions, olfactory disorders and sleep disturbances. The pharmacological and non-pharmacological treatment options for Parkinson's disease have improved considerably over the years. In recent years it has also been possible to improve the mobility by electrical stimulation of the basal ganglia. We have had experience in the field of deep brain stimulation for more than 20 years.
Torticollis - dystonia

Dystonia describes a movement disorder that leads to involuntary tensioning of individual muscles or muscle groups. This causes contractions and malpositions, and related limitations of the voluntary movements of the affected body region. Spasmodic torticollis and blepharospasm are frequent examples of dystonia. Dystonic movement disorders can very effectively be treated with injections of botulinum toxin into the affected muscles (please also see botulinum toxin treatment). Generalized dystonia can also be treated with deep brain stimulation.
Dementia
Dementia is the progressive loss of cognitive and intellectual abilities as a result of an acquired disease of the brain in people who previously had an unremarkable mental development. The reduction in cognitive performance inevitably entails an increasing decline in everyday, occupational and social activities. The frequency of dementia increases at an older age.
The American Institute on Aging has formulated seven warning signs that may indicate incipient Alzheimer's disease, and which should induce people in the immediate environment to seek medical advice:
- The ill person repeats the same question over and over again.
- The ill person tells the same short story over and over again.
- The ill person no longer knows how everyday activities, such as cooking, playing cards, handling the remote control, work.
- The ill person has forgotten how to handle money, transfers, bills and the like safely.
- The ill person no longer finds many objects or puts them in unusual places (unintentional hiding) and suspects other people of having taken away the missing object.
- The ill person persistently neglects his/her appearance, but denies it.
- The ill person answers questions repeating the question put to him/her.
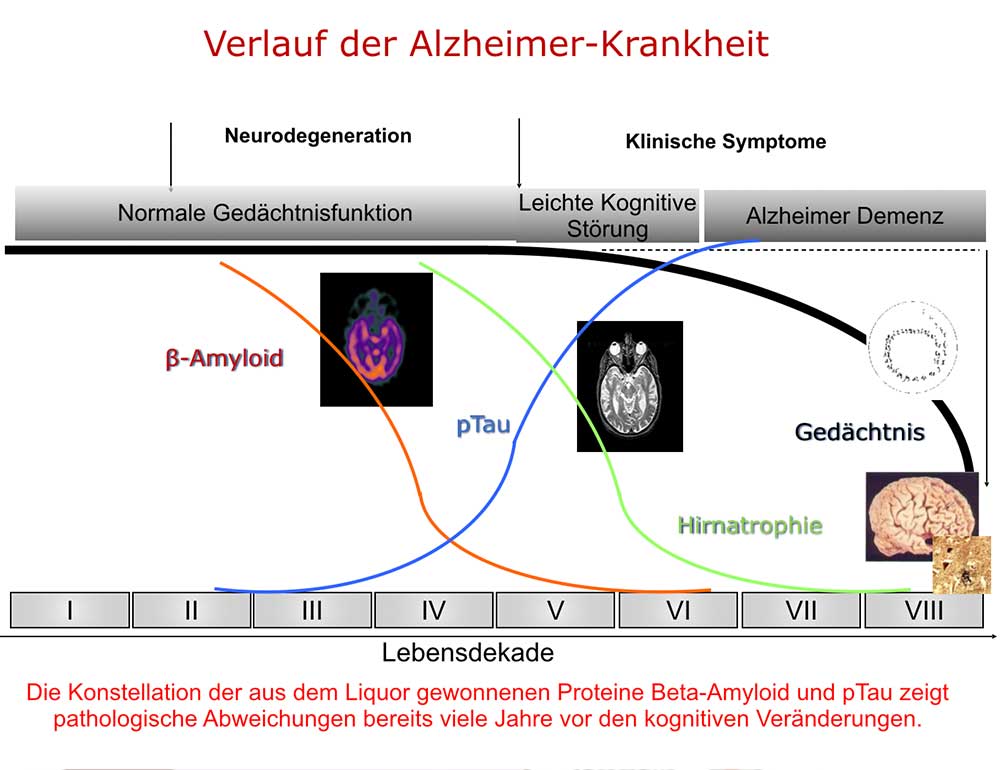 Early detection of a certain protein constellation in the cerebrospinal fluid (CSF) by means of a cerebrospinal fluid puncture (s. below) can be achieved many years before the occurrence of the first symptoms. This will allow prophylactic measures to be taken at an early stage. Physical and mental training are important for the prevention of a dementia process. New studies have shown that a deterioration of the brain can be achieved by a special combination of nutritional supplements (Soininen H, Solomon A, Visser PJ, et al. 36-month LipiDiDiet multinutrient clinical trial in prodromal Alzheimer’s disease. Alzheimer’s Dement. 2021; 17:29–40. Link: https://doi.org/10.1002/alz.12172).
Early detection of a certain protein constellation in the cerebrospinal fluid (CSF) by means of a cerebrospinal fluid puncture (s. below) can be achieved many years before the occurrence of the first symptoms. This will allow prophylactic measures to be taken at an early stage. Physical and mental training are important for the prevention of a dementia process. New studies have shown that a deterioration of the brain can be achieved by a special combination of nutritional supplements (Soininen H, Solomon A, Visser PJ, et al. 36-month LipiDiDiet multinutrient clinical trial in prodromal Alzheimer’s disease. Alzheimer’s Dement. 2021; 17:29–40. Link: https://doi.org/10.1002/alz.12172).
A frequent cause of dementia is Alzheimer's disease and poor blood supply to the brain (vascular dementia), but there is also a series of other diseases that can be the cause of dementia. A series of standardized tests can be used to determine whether a cognitive performance disorder, such as increased forgetfulness, is a result of dementia-related brain disease.
The therapy of dementia primarily depends on the cause: If dementia is the consequence of another disease, such as an infection, a metabolic disorder or depression, it can be treated as part of the treatment of this underlying disease. In the meantime, however, there are also pharmacological therapies for Alzheimer's disease and vascular dementia which, although they do not lead to a cure, do effectively delay the decline in cognitive performance.
The course of the disease is divided into different stages, each of which focuses on other physical and mental limitations.
Multiple sclerosis
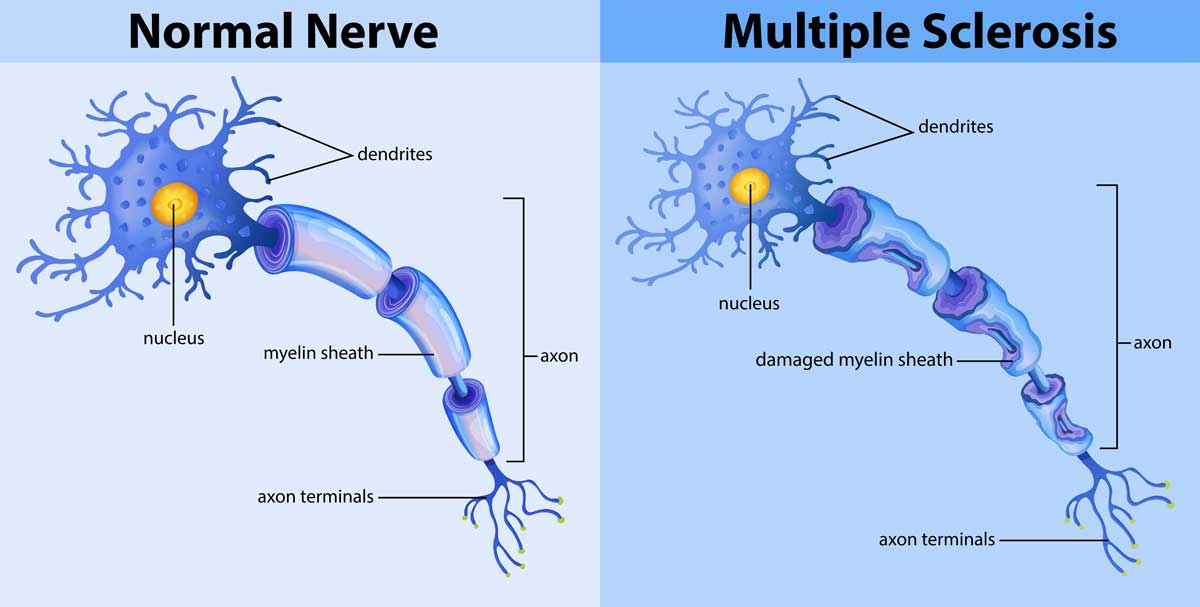 Multiple sclerosis (MS) or encephalomyelitis disseminata (ED) is a chronic-inflammatory neurological disease with different forms, which is why it is dubbed with the term "the disease with a thousand faces". It affects the myelin sheaths, the electrically insulating outer layer of nerve fibers in the central nervous system (CNS).
Multiple sclerosis (MS) or encephalomyelitis disseminata (ED) is a chronic-inflammatory neurological disease with different forms, which is why it is dubbed with the term "the disease with a thousand faces". It affects the myelin sheaths, the electrically insulating outer layer of nerve fibers in the central nervous system (CNS).
Thus, a functional disorder and tissue damage occur, which are associated with a great number of complaints, such as visual disorders, palsies, and sensory disturbances. The disease usually appears between the ages of 20 and 40. It usually has an intermittent course and is slow in progress. The cause of this disease has not been fully clarified. A disorder of the immune system in the form of a so-called autoimmune disease is suspected. In recent years in particular, the therapeutic options have improved dramatically.
We have the possibility of diagnosis by means of imaging procedures, electrophysiology, laboratory, and lumbar puncture.
Acute treatment
In the case of an acute flare with neurological signs lasting for more than 12 hours, a neurological examination should be performed as soon as possible and immediate treatment be provided. We have a day-care bed in our practice and occupancy beds in a private hospital (Clínica Juaneda)
Preventive treatments
There are numerous drugs used as first-line basic therapy in multiple sclerosis outbreak prophylaxis to reduce the frequency and severity of acute inflammatory flares. The same drugs as those used in other EU countries are available in Spain. However, they are generally supplied exclusively through hospital pharmacies and require a physician's prescription and a report on the indication. We cooperate with the pharmacy in our admitting hospital Clínica Juaneda.
Individual complaints that occur in multiple sclerosis can be positively influenced by different measures, e.g. medication, intrathecal treatment, or Botox against spastic symptoms, pain, bladder voiding disturbances, and fatigue. In the case of spasticity and movement disorders, our Department of Physiotherapy is available to you.

Peripheral nerve damage
A damage to the peripheral nervous system can be detected by an electrophysiological examination (s. below). Peripheral nerve damage and its consequences include, among others:
- disc diseases,
- bottleneck and pressure injuries,
- carpal tunnel syndrome,
- ulnar groove syndrome,
- peroneal palsy,
- tarsal tunnel syndrome,
- Polyneuropathy
Polyneuropathy is a damage to the so-called peripheral nervous system. This is a dysfunction of the nerves in the arms and legs, the symptoms frequently starting in the feet, and less frequently also in the hands. The complaints are frequently accompanied by paresthesia in the relevant limbs. Sensory disorders or muscle weakness may occur. We use the entire electrophysiological diagnostic methods, also further laboratory, and cerebrospinal fluid tests if necessary, in order to diagnose this group of diseases. - Neuropathic pain
Neuralgic pain is also frequently triggered by neuropathies. An individually coordinated pain therapy can mostly help the affected person to reduce the pain to a tolerable level and significantly increase the quality of life.

Epilepsy
The nerve cells and their interaction are controlled by electric impulses. Only by means of a regulated interaction are we able to think, feel, move, or absorb sensations, such as light or music. Any disturbances of this system can cause very different complaints or diseases, among others, epileptic seizures.
Epilepsy is a disease with very different manifestations. What all forms have in common is that seizures that are triggered by brain dysfunction occur from time to time. Besides a congenital predisposition to seizures, epileptic seizures, i.e. electrical failures in the brain, can be caused by injuries due to accidents, damage due to a tumor or, for example, alcohol, inflammation, cerebral hemorrhage or circulatory disorders. The electroencephalogram (EEG) is considered as the most important method of examination in the case of seizure disorders.
Sleep disorders
People with disturbed sleep often feel left alone with their disturbance while everyone else gets a good night's sleep. They are often troubled by the thought that they have suffered from insomnia for years, have tried many things, nothing has helped properly or only temporarily, and instead other problems such as medication abuse may possibly have been added. What is especially incomprehensible for most of the affected people is that the sleep disorder is taken for granted after some time.
Here you will soon find two self-assessment sheets that can give clues about the nature and cause of the sleep disorder. After a detailed examination, we can detect most causes of a sleep disorder in our sleep laboratory.
Restless legs syndrome
The restless legs syndrome (RLS) refers to a movement disorder which is characterized by sensory disturbances and an urge to move primarily in the lower extremities (less frequently also in the arms). Painful sensations frequently exist that can only be relieved by movements. RLS is occasionally associated with involuntary movements and or periodic leg movements (PLM) while sleeping. These symptoms increase at rest and during the night, while they are less pronounced during the day and while moving. It is usually diagnosed on the basis of the medical history and can be confirmed in the sleep laboratory. Here you will soon find a self-assessment sheet regarding this syndrome.
